Unfortunately, sometimes we feel like we’re hitting our head against the wall when trying to answer these questions.
Photo by Daniel Mingook Kim on Unsplash
Each one of these questions are so important, and for some, this might seem like a life sentence. But… What if I told you knee arthritis isn’t bad? Arthritis is a normal part of life, and an ageing process that each and every one of us have to go through as we age.
There are so many uncontrollable factors that influence the onset of arthritis, from:
It doesn’t seem so bad now does it?
We’ve all heard that arthritis is bad. That it’s this disastrous diagnosis spelling the end of our youth and that we have old and painful, arthritic joints. But the thing is, arthritis and pain are not mutually exclusive. What I mean is that: You can have a diagnosis of knee arthritis, and have pain… But you can also have a diagnosis of knee arthritis, and have no pain!
Confused yet?
The fact is that research supports the notion that osteoarthritic changes occurs in everyone. However, there are also individuals that have severe levels of joint arthritis, but are completely asymptomatic and have no pain (Dieppe & Lohmander, 2005).
Which means that arthritis DOES NOT equal pain. Please repeat that after me – Arthritis DOES NOT equal pain.
The good thing is, while we cannot fix your knee arthritis (because our medical and technological advancements aren’t at this stage), we can perform some simple actions and steps to relieve your pain. These are split into two main categories.
These techniques involve massaging or ‘trigger point release’ of the ‘tight’ musculature around the hip and knee joint, which may be involved in the tight sensation and painful feelings in these muscles. Fundamentally, massage does not change the underlying structures or physiology of muscles, nor does it make you any stronger, or place you in any position to decrease long-term outcomes by any means.
Regardless, they are still fantastic for pain relief. Trigger points and massaging of the common sensitive areas including: glute medius (side of your hip), glute max (your buttocks), your hamstring origin into the ischial tuberosity (the bony part of your bum) as well as the quadriceps (your thigh muscles).



As for duration and prescription – there are no strict guidelines as to how long you should spend on one specific area. The easiest way to approach this is:
Be cautious of being over eager with massage, as you may find a bit more bruising the next day!
Passive stretching is also a fantastic way to create some quick pain relief for tight structures and painful areas. However, while a long term stretching program may be able to increase flexibility or range, it does not increase the strength or stiffness of your muscles and tendons (Marshall, Cashman & Cheema, 2011). This may predispose the muscle or the individual to recurrent injury and may not provide any long term benefits.
Again, stretching is a fantastic adjunct or add-on to the next few steps, but should never be on its own. Some example stretches for the knee may include general quadriceps and hamstring stretches, glute med stretch (newspaper stretch), and calf stretching.






General prescriptions for stretching exercises generally vary around 20 – 30 second holds, for 2 – 3 sets of each stretch. I wouldn’t spend a lot of time stretching as there are other strategies and movements that can provide much greater benefits than stretching alone.
Understand that your pain is a multifaceted, complex machine. Simply attributing pain to the results shown on a scan is vastly underestimating the complexity of pain. Instead, we should be learning how to manage and understand the difference between “good” and “bad” pain.
We must understand that pain does not necessarily equate to structural damage within the knee. This is especially important as many are worried about further long-term damage when there is any onset of pain, especially with a diagnosis of knee arthritis. This can lead into negative habits and beliefs, and can have long-term consequences as a result.
A simple and easy way to understand this would be using “the pain cycle. “The cycle is destructive, and usually starts with pain, then immobility (decreased movement), atrophy (loss of muscle), decreased function which creates a predisposition for pain and the cycle starts again (Figure 1).
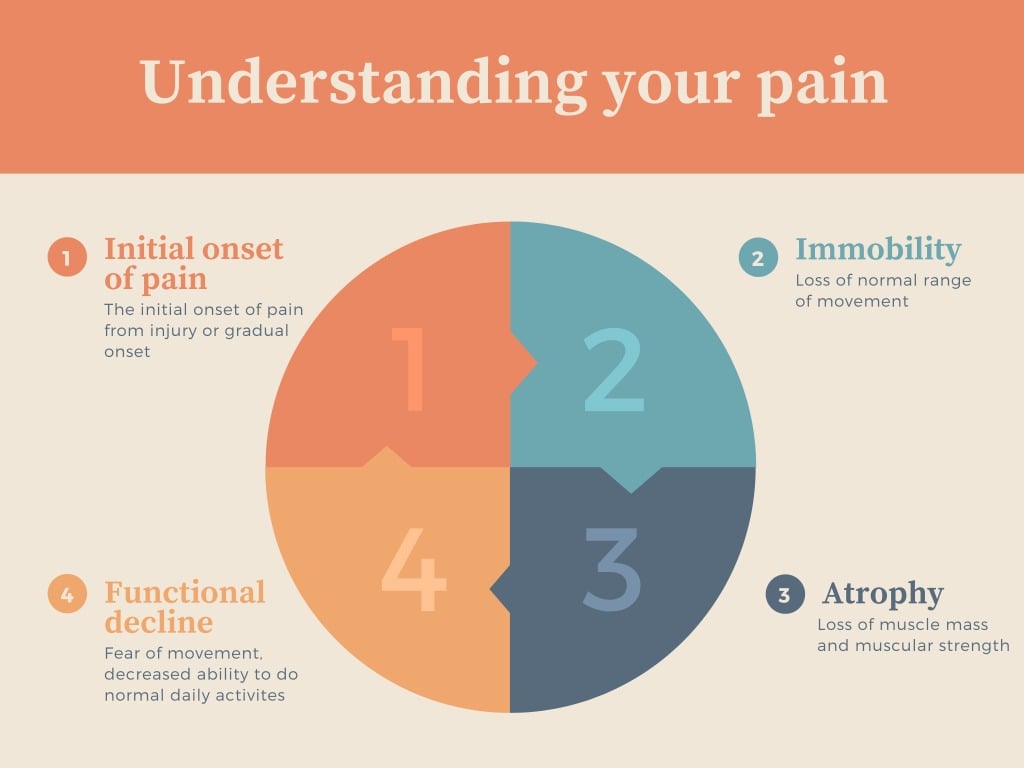
Figure 1: The pain-function cycle
Ultimately, our aim is to be able to intercept this pain cycle at one or multiple parts. Either through strengthening, encouraging movement and healthy practices, or – in extreme circumstances – the use of pain medication to offset the pain just enough that we can engage in exercises.
Long-term improvement and prevention requires a structured exercise program aimed at targeting the specifically weak muscles of your lower limb. These exercise programs include strengthening of the glutes, quadriceps, hamstrings, calves and even your feet.
Exercise prescription is in itself a huge topic and one that I will save for a later blog post. However, general suggestions to improve lower limb strength and provide some basic strengthening for the lower limbs include: glute bridges, elevated glute bridges, calf raises as well as step ups.









Prescription for these can vary from 10 – 20 reps, 2 – 3 sets depending on your current fitness activity levels as well as your pain levels. If you are worried about rising or fluctuating pain levels, a set of rules that you can follow is, if your pain:
Then STOP. You may have done too much, and will need to ramp it down and monitor your situation. Exercise prescription is a delicate balance between finding just enough exercise to help stimulate strengthening while also not performing too much that it stirs it up and makes it annoying unbearable to walk or move on.
Many individuals will have been plagued by knee pain or fear of knee osteoarthritis for years and years. Worse still, some individuals have been given the diagnosis of “knee arthritis” and were never given any actionable steps or solutions to easing pain and improving movement. The aim of this post is to highlight the fact that knee osteoarthritis is not a ‘death sentence,’ and we should not be overly worried about the ramifications brought about by scans and investigations and by even the words of some medical professionals.
Short-term treatments for pain may include massage, ‘self-myofascial release’, trigger points and stretches. However, if we are aiming for long-term improvement and prevention of pain in the knee, then understanding your pain is paramount and being able to provide a structured exercise program is key.
For more information, keep following our blogs for weekly posts.
Don’t hesitate, book in a consultation and talk to us!
If you could start moving again and get rid of your knee pain, how would that affect your life?